MEDICINE BLOG
MEDICINE BLOG:
-108 Koushik








This is an online e-log platform to discuss case scenario of a patient with their guardians permission.
I have been given this case to solve in an attempt to understand the topic of patient clinical data analysis to develop my competency in reading and comprehending clinical data including, history, clinical findings ,investigations, come up with a diagnosis and treatment plan.
A 47 yr old male from lingotam driver by occupation came to OPD on 18/06/2023 with chief complaints of:
-unresponsiveness since 5:00 AM on 18/06/2023
-Burning sensation on passing urine since 3 days
- profuse sweating since 5:00 AM on 18/06/2023
History of presenting illness:
Patient was apparently asymptomatic before 5:00 AM on 18/06/2023 then when he was going to washroom he had a dizzy feeling and fell to the ground and he was in a unresponsive state.
His wife then called RMP doctor and he suggested to give him some sugar,then was brought to casualty.
History of similar complaint one week ago and came to the casualty and he didn't want to get admitted into the hospital.
Patient complained of burning micturiton since 3 days.
No complaints of fever,cold,cough,vomiting,loose stools.
No complaints of shortness of breath,chest pain,palpitations,orthopnea,pnd.
Past history:
History of similar complaint one week ago and came to the casualty and he didn't want to get admitted into the hospital.
Patient is a known case of diabetes since 10 years.
Not a known case of Hypertension,epilepsy ,tuberculosis,asthma,cad,pedal edema,facial puffiness.
Family history:
No significant family history
Personal history:
Marital status: married
Sleep: adequate
Diet: mixed
Appetite:normal
Bowel and bladder:regular and normal
Addictions: Smoking since 20 years 10 cigarettes per day
Daily routine:
Patient wakes up at 5:00 AM and goes for washroom then he sleeps again.
Then he wakes up again at 6:00 gets fresh and eats breakfast by 7 AM.
Then he takes formin SR 500 mg tablet
He is not going for work since 6 months
Aft by 12-1 PM he eats rice and vegetables dal occasionally
Then he sleeps till evening
Drinks tea in the evening
Has dinner by 8:00 PM
Sleeps by 9:00 PM
Surgical history :
No significant surgical history
Treatment history:
Formin SR 500 daily once since 10 years
General examination:
Patient was conscious,coherent, cooperative well oriented to time,place and person
No pallor,icterus,cyanosis,clubbing, lymphadenopathy,pedal edema
Vitals:
Temperature: Afebrile
Pulse: 84 BPM
RR:16 cycles/min
BP: 110/80 mmHg
Systemic examination:
CVS:
S1,S2 HEARD
NO MURMERS
Respiratory system:
Trachea Central in position
B/L air entry present
Normal vesicular breath sounds heard
Per abdomen:
Abdomen : scaphoid
Spleen non palpable
Liver non palpable
No tenderness
CNS:
No focal neurological deficit found
Sensory:normal
Motor: normal
Bulk:Right arm :25 cm
Left arm : 25 cm
Right forearm: 22 cm
Left forearm: 24 cm
Right proximal muscles:33 cm
Left proximal muscles: 33 cm
Right distal muscles:29 cm
Right distal muscles:29 cm
Cranial nerves: normal
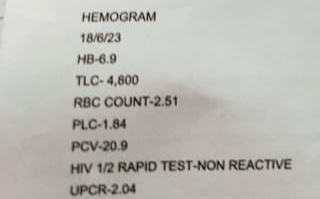
Investigations:






Reports:
Provisional diagnosis:
Induced hypoglycemia secondory to oral hypoglycemic drugs
Treatment:
Inj.25D 100 ML IV STAT
STOP OHA till further notice
GRBS MONITORING
Comments
Post a Comment